Narciso F. Atienza, Jr. MD, MBA, DPBO
EYE PHYSICIAN AND SURGEON
DIPLOMATE, PHILIPPINE BOARD OF OPHTHALMOLOGY
SUBSPECIALTY IN DISEASES AND SURGERY OF THE RETINA, VITREOUS, AND MACULA and OCULAR ONCOLOGY
DIPLOMATE, PHILIPPINE BOARD OF OPHTHALMOLOGY
SUBSPECIALTY IN DISEASES AND SURGERY OF THE RETINA, VITREOUS, AND MACULA and OCULAR ONCOLOGY

What is ARMD?
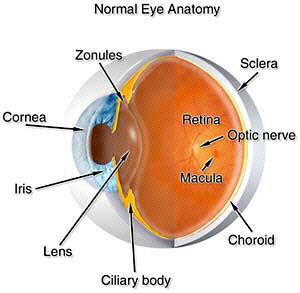
Age related macular degeneration (ARMD) is one of the most common causes of vision loss in patients more that 60 years old. This happens when the small blood vessels inside the eye begins to harden, which is usually associated with aging. The hardening causes the amount of oxygen and nutrients to decrease, causing the macula, the most active part of the retina, to loss function and hence central vision. This can be detected long before vision loss would occur
Severity of ARMD varies widely. In worst cases, there is complete loss of central vision, making reading or driving impossible. For others, it only causes slight distortion. However, macular degeneration does not cause total blindness since it does not usually affect the peripheral vision. There are 2 types of Age Related Macular Degeneration, the wet type (neovascular) and the dry type (non-neovascular).
What is the difference between wet and dry macular degeneration?
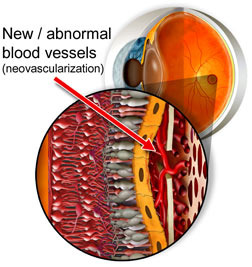
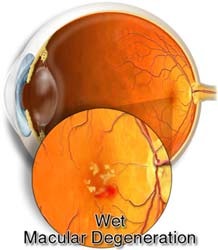
AMD is classified as either wet (neovascular) or dry (non-neovascular). About 10% of patients who suffer from macular degeneration have wet AMD. This type occurs when new vessels form to improve the blood supply to oxygen-deprived retinal tissue. However, the new vessels are very delicate and break easily, causing bleeding and damage to surrounding tissue.
Patient with wet macular degeneration develop new blood/abnormal vessels under the retina. This causes hemorrhage, swelling, and scar tissue but it can be treated with laser in some case.
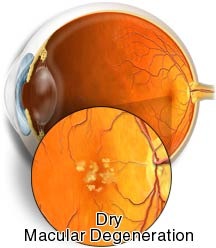
Dry macular degeneration, although more common, typically results in a less severe, more gradual loss of vision. In this type of macular degeneration, there is the formation of small lesions called drusen, which are actually deposits from the metabolism of cells of the retina. This lesions causes the macula to lose function.
What causes macular degeneration?
Macular degeneration may be caused by variety of factors. Genetics, age, nutrition, smoking, and sunlight exposure may all play a role.
What are its’ signs and symptoms?
Loss of central vision. This may be gradual for those with the dry type. Patients with the wet type may experience a sudden decrease of the central vision, or difficulty reading or performing tasks that require the ability to see detail. Distorted vision (Straight lines such as a doorway or the edge of a window may appear wavy or bent.)
Detection and Diagnosis
Eye physicians usually diagnose AMD. Vision testing, Amsler grid test, ophthalmoscopy, fundus photography, OCT and fluorescein angiography are some common tests performed during a retinal exam.
Treatment
There is no proven medical therapy for dry macular degeneration. In selected cases of wet macular degeneration, laser photocoagulation is effective for sealing leaking or bleeding vessels. Unfortunately, laser photocoagulation usually does not restore lost vision, but it may prevent further loss. Photodynamic therapy has proven to be effective in stopping abnormal blood vessel growth in some patients with wet AMD. This new type of laser treatment is far less damaging than laser photocoagulation and is the treatment of choice in many cases.
The standard of care nowadays is the injection of anti-VEGF (vascular endothelial growth factor) medications to arrest the growth of the new blood vessels causing the macular degeneration by acting against the chemical causing the new growth. These medications (Macugen, Pegaptanib, Pfizer) (Lucentis, Ranibizumab, Novartis, Genentech) (Eylea, Aflibricept, Regeneron Bayer) have been FDA approved for neovascular macular degeneration.
Cataract surgery done if you have advanced age related macular degeneration may not improve your vision too much, and it may even cause deterioration of vision over time.
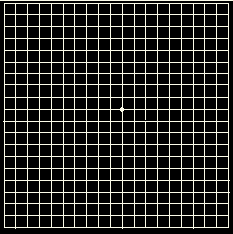
Early diagnosis is critical for successful treatment of wet macular degeneration. Patients can help the doctor detect early changes by monitoring vision at home with an Amsler grid.
Nutrition and macular degeneration
Several recent studies have indicated a strong link between nutrition and the development of macular degeneration. It has been scientifically demonstrated that people with diets high in fruits and vegetables (especially leafy green vegetables) have a lower incidence of macular degeneration. The Age Related Eye Disease Study (AREDS) concluded at the following nutrients: 500 milligrams of vitamin C; 400 International Units of vitamin E; 15 milligrams of beta-carotene (often labeled as equivalent to 25,000 International Units of vitamin A); 80 milligrams of zinc as zinc oxide; and two milligrams of copper as cupric oxide are recommended to halt the progression of dry-type macular degeneration. Beta-Carotene must be used with caution on smoking patients as there is an increase in risk of developing lung cancer with patients who smoke and take Beta-Carotene. The role of lutein/zeaxanthin + omega 3 fatty acids been studied in AREDS 2. Results show that adding omega 3 fatty acids + lutein/zeaxanthin to the original formula of AREDS do not alter the progression of AMD, however, lutein/zeaxanthin may be of some benefit as replacement for beta-carotene for AMD patients who are smoking or who have had a history of smoking.
Is ARMD associated with systemic diseases?
Though there is no definite proof, more hypertensive patients have ARMD compared to non-hypertensive patients. This is said to be due to the small vessel changes in hypertension.
Smoking also is associated with patients with ARMD, hence, smokers with ARMD are advised to stop the habit.
Age related macular degeneration (ARMD) is one of the most common causes of vision loss in patients more that 60 years old. This happens when the small blood vessels inside the eye begins to harden, which is usually associated with aging. The hardening causes the amount of oxygen and nutrients to decrease, causing the macula, the most active part of the retina, to loss function and hence central vision. This can be detected long before vision loss would occur
Severity of ARMD varies widely. In worst cases, there is complete loss of central vision, making reading or driving impossible. For others, it only causes slight distortion. However, macular degeneration does not cause total blindness since it does not usually affect the peripheral vision. There are 2 types of Age Related Macular Degeneration, the wet type (neovascular) and the dry type (non-neovascular).
What is the difference between wet and dry macular degeneration?
AMD is classified as either wet (neovascular) or dry (non-neovascular). About 10% of patients who suffer from macular degeneration have wet AMD. This type occurs when new vessels form to improve the blood supply to oxygen-deprived retinal tissue. However, the new vessels are very delicate and break easily, causing bleeding and damage to surrounding tissue.
Patient with wet macular degeneration develop new blood/abnormal vessels under the retina. This causes hemorrhage, swelling, and scar tissue but it can be treated with laser in some case.
Dry macular degeneration, although more common, typically results in a less severe, more gradual loss of vision. In this type of macular degeneration, there is the formation of small lesions called drusen, which are actually deposits from the metabolism of cells of the retina. This lesions causes the macula to lose function.
What causes macular degeneration?
Macular degeneration may be caused by variety of factors. Genetics, age, nutrition, smoking, and sunlight exposure may all play a role.
What are its’ signs and symptoms?
Loss of central vision. This may be gradual for those with the dry type. Patients with the wet type may experience a sudden decrease of the central vision, or difficulty reading or performing tasks that require the ability to see detail. Distorted vision (Straight lines such as a doorway or the edge of a window may appear wavy or bent.)
Detection and Diagnosis
Eye physicians usually diagnose AMD. Vision testing, Amsler grid test, ophthalmoscopy, fundus photography, OCT and fluorescein angiography are some common tests performed during a retinal exam.
Treatment
There is no proven medical therapy for dry macular degeneration. In selected cases of wet macular degeneration, laser photocoagulation is effective for sealing leaking or bleeding vessels. Unfortunately, laser photocoagulation usually does not restore lost vision, but it may prevent further loss. Photodynamic therapy has proven to be effective in stopping abnormal blood vessel growth in some patients with wet AMD. This new type of laser treatment is far less damaging than laser photocoagulation and is the treatment of choice in many cases.
The standard of care nowadays is the injection of anti-VEGF (vascular endothelial growth factor) medications to arrest the growth of the new blood vessels causing the macular degeneration by acting against the chemical causing the new growth. These medications (Macugen, Pegaptanib, Pfizer) (Lucentis, Ranibizumab, Novartis, Genentech) (Eylea, Aflibricept, Regeneron Bayer) have been FDA approved for neovascular macular degeneration.
Cataract surgery done if you have advanced age related macular degeneration may not improve your vision too much, and it may even cause deterioration of vision over time.
Early diagnosis is critical for successful treatment of wet macular degeneration. Patients can help the doctor detect early changes by monitoring vision at home with an Amsler grid.
Nutrition and macular degeneration
Several recent studies have indicated a strong link between nutrition and the development of macular degeneration. It has been scientifically demonstrated that people with diets high in fruits and vegetables (especially leafy green vegetables) have a lower incidence of macular degeneration. The Age Related Eye Disease Study (AREDS) concluded at the following nutrients: 500 milligrams of vitamin C; 400 International Units of vitamin E; 15 milligrams of beta-carotene (often labeled as equivalent to 25,000 International Units of vitamin A); 80 milligrams of zinc as zinc oxide; and two milligrams of copper as cupric oxide are recommended to halt the progression of dry-type macular degeneration. Beta-Carotene must be used with caution on smoking patients as there is an increase in risk of developing lung cancer with patients who smoke and take Beta-Carotene. The role of lutein/zeaxanthin + omega 3 fatty acids been studied in AREDS 2. Results show that adding omega 3 fatty acids + lutein/zeaxanthin to the original formula of AREDS do not alter the progression of AMD, however, lutein/zeaxanthin may be of some benefit as replacement for beta-carotene for AMD patients who are smoking or who have had a history of smoking.
Is ARMD associated with systemic diseases?
Though there is no definite proof, more hypertensive patients have ARMD compared to non-hypertensive patients. This is said to be due to the small vessel changes in hypertension.
Smoking also is associated with patients with ARMD, hence, smokers with ARMD are advised to stop the habit.